Doc, what happens if I calculate the burn area wrongly? Is it
really important?
Arthur A, Canada
As we have seen in
previous posts the loss of fluid from the skin surface depends on the degree of
burns and the area of the burns. One must evaluate the total burn surface area
(TBSA) to calculate the fluid requirements. There are different methods of
fluid calculation in burns.
a) Rule of nine
The rule of nine works
well in adult patients. In this method the body surface is divided into various
parts measuring in nines.
Rule of nine
Each arm - 9% TBSA
Head - 9% TBSA
Anterior thorax - 18%
TBSA
Posterior thorax - 18%
TBSA
Perineum - 1% TBSA
Each leg - 18% TBSA
Any burn surgeon will tell you that more
often the burns are so irregularly placed that accurate calculation becomes
difficult in different regions of the body. In such cases a simple trick is to
use the palm of the hand as a method of calculation. At any age the palm of the
hand is approximately 1% and can be used to measure the burn areas. One must not forget that it is the patient’s
hand that is used for the calculation and not the doctor’s. An approximate size
of the palm of the patient is considered and the equivalent burn area is
estimated. For e.g. lets say the burn area was 5 palm sizes of the patient over
the body and lower limbs. Now we can assume that the patient has about 5% burns.
It should be noted that first degree
burns do not produce fluid losses and therefore only 2nd degree
burns or more should be used for fluid calculation.
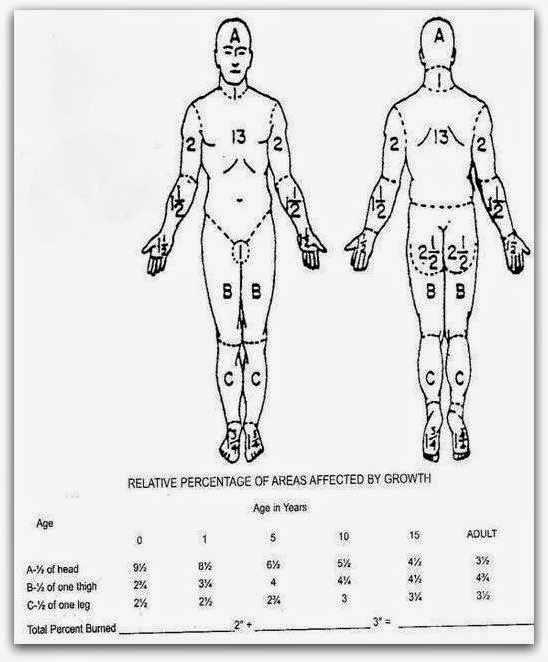
However in children the rule of nine
can lead to serious errors as the head and body is larger in TBSA than the
limbs and therefore the Lund and Browder charts work out to be
more accurate while calculating the fluids to be administered. The Lund and Browder chart is shown below.
If the fluid calculation is wrong
then the patient will be administered less fluids and this will result in shock
or low volume circulatory failure and ultimately may be fatal. The fluids calculated need to be replaced
within a time limit as we shall discuss in the next post. Correct volume replacement
and correct timing is what makes the resuscitation of burns patients
successful.
(an original initiative in burn care and education from
asktheburnsurgeon+)

