Doc, besides actually looking and evaluating the burn area is there other
ways of knowing that the burn area might be deep?
Marjorie A, Sidney, Australia
A
number of factors should be considered while evaluating the burn depth- temperature
at which the burn is caused, duration of contact, cause of burn and site of
burn.
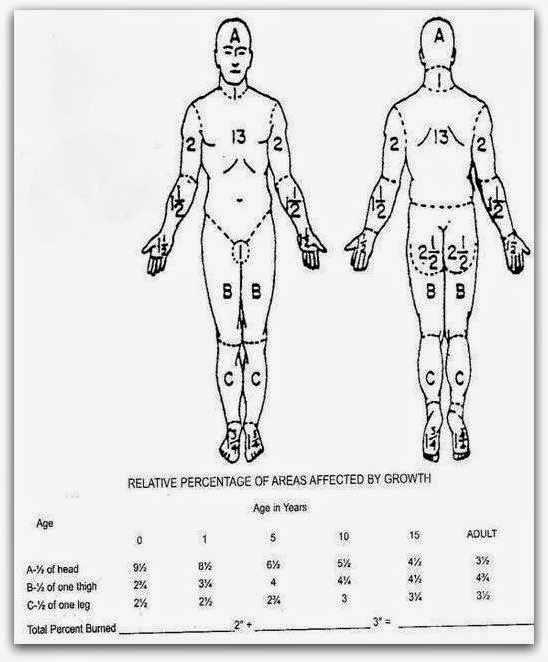
The
area which is burnt is also important as the skin thickness varies at different
sites (from 1 mm in the genitalia and eyelids to 5 mm in palms and soles). The skin is relatively thinner in children and
geriatric patients and therefore they tend to suffer a greater degree of burns.
Contact
burns tend to be deeper since the burning object or the hot object like the exhaust
of a motorcycle remains in direct contact and causes more damage to the skin.
It must be noted that the lesser the duration
of the burn, the lesser the degree of burn. Therefore it is recommended that
the burn area be cooled at the earliest. Pouring cold water over burns areas
works on this principle and one must within seconds carry out this maneuver to
avoid severe burns. The home kitchen is one area where burns often occur. Fortunately
water is always available in the kitchen and therefore quickly pouring cold or
tap water over the burn area works wonders and one should let the cold water
run over the burn area for a few minutes.
Application
of oil or mint preparations as is often done by lay people should be avoided as
oil stops the heat loss from the surface causing more damage and mint just
gives cools the mind and not the burn area.
The
cause of the burn should be inquired into as different modes of burns can cause
different depths of burns. For e.g. hot water burns are less deep than hot frying
pan oils, as the temperatures of hot oil touch 175-200 degrees compared to hot
water which may be 75-100 degrees. Different acids and bases can cause
different degree of burns depending on their strengths. Thus knowing the burn agent helps a lot in deciding the depth of the burn and predicting the outcome.
We shall discuss how the monitor burn patients in our next post....
(An original initiative in burn care and education from asktheburnsurgeon++)